Got the denial letter today? You have 180 days. 80% of appealed prior-auth denials are overturned — fewer than 1% try.See your 30-minute plan →
Patient Evidence · United States
··11 min read
Denied for Zepbound, IVF, or a $34K surgery bill? Appeal it this weekend.
80% of appealed prior-auth denials are overturned. Fewer than 1% of patients try. Counterforce Health drafts the appeal letter free in minutes. The reason most appeals still lose is the same reason Cigna can deny 300,000 claims at 1.2 seconds each: nobody can prove what their portal said. ProofSnap is the $4.99 evidence layer that fixes that.
How to appeal a US health insurance denial in 2026
To appeal a denied health insurance claim in the United States, follow five steps: (1) read the denial letter and identify the appeal deadline — 180 days for ACA marketplace and Aetna / BCBS / Cigna / Premera commercial plans, 65 days for UnitedHealthcare, 60 days for Humana and all Medicare Advantage plans; (2) request your full medical records and prior-authorization correspondence under HIPAA right of access (45 CFR 164.524); (3) draft the appeal letter using a free AI tool such as Counterforce Health (~70% reported overturn rate, University of Pennsylvania / NIH funded); (4) attach court-admissible authenticated evidence of the portal page, EOB, and prior-auth approval — a plain phone screenshot is not enough under Federal Rules of Evidence 901(a); (5) submit the internal appeal, then escalate to external review (IRO) within 4 months if denied.
80%
Of appealed prior-auth denials overturned (CMS, AMA)
ProofSnap is not your appeal letter. It is the evidence layer that makes the appeal win.
Find your situation below. The right next step depends on which fight you are actually in.
Stage 1First denial
"I just got my first denial letter."
Start with the free AI tool that drafts the appeal letter for you. Then capture the denial letter, prior-auth approval, and portal status with ProofSnap so the insurer cannot quietly change the record while you wait for the IRO review.
"I lost my appeal — and the portal looks different now."
This is exactly what ProofSnap was built for. Insurers change portal content, archive prior-auth letters, and edit chat transcripts. Your screenshot is not enough for an IRO or bad-faith case. You need authenticated, blockchain-timestamped evidence to escalate.
Patient advocate, claims advocate, ERISA / bad-faith / malpractice attorney, or healthcare power-of-attorney. With written client authorization you have the same record-access rights as the patient. Subscription plans cover unlimited client captures with full chain-of-custody for litigation.
Not sure? If you have not yet appealed, start with Counterforce Health (free) for the letter and SnapPack ($4.99) for the evidence. If your first appeal failed, ProofSnap captures are the difference between losing the IRO and winning it.
Documented US cases — not hypotheticals
When the portal forgets, the patient pays — sometimes with their life
Seven cases from federal court filings, ProPublica investigations, and major US outlets. Each one ends with a patient who could not prove what the insurer or chart said before it changed. Each is exactly the failure mode a $4.99 SnapPack closes.
Cigna PXDX — 300,000 claims denied in two months
ProPublica, March 2023
Cigna's PXDX ("procedure-to-diagnosis") system let company doctors deny claims in batches with electronic signatures — on average 1.2 seconds per claim, never opening a file. One medical director, Dopke, rejected 121,000 claims in two months. Class actions filed in California and Connecticut have been allowed to proceed.
UnitedHealth nH Predict — AI cut off elderly nursing-home patients
Estate of Lokken v. UnitedHealth Group, D. Minn., 2023–present
A federal class action alleges UnitedHealth used the nH Predict algorithm to override physician recommendations and cut Medicare Advantage post-acute care short. Internal data shows over 90% of appeals were overturned — but the insurer relied on the fact that only ~0.2% of patients ever appeal. In March 2026 a federal magistrate ordered broad discovery into the AI denial pipeline.
EviCore (Evernorth/Cigna) screens prior-auth requests for Cigna, UnitedHealthcare, Aetna and Blue Cross plans covering 100 million Americans. Internal documents describe an algorithm called "the dial" tuned to increase the denial rate by 15%. ProPublica documented 30 inappropriate cancer denials traced to outdated guidelines.
Aetna medical director: "I never read the records."
Washington v. Aetna (CA), 2018 deposition
Dr. Jay Iinuma, Aetna's medical director for Southern California 2012–2015, testified under oath that he never reviewed patients' medical records when deciding to approve or deny care — he relied entirely on nurses' summaries. The case was brought by 23-year-old Gillen Washington, denied IVIG infusions for a rare immune disorder. California's insurance commissioner opened a state-wide investigation; Aetna settled before trial.
Nataline Sarkisyan, 17 — died hours after Cigna reversed the denial
December 2007, Glendale CA
Cigna denied coverage for a liver transplant Nataline's doctors at UCLA Medical Center said was medically necessary after complications from a bone-marrow transplant. After public pressure and a nurses-union protest, Cigna reversed the decision on Dec 20, 2007. Nataline died a few hours later, before surgery could be performed. The family's wrongful-death suit reshaped the US health-reform debate.
McNaughton v. UnitedHealthcare, E.D. Pa. 2021–2023
A Penn State student with crippling ulcerative colitis sued UnitedHealthcare after it refused to cover the Mayo Clinic-prescribed regimen finally working for him. Discovery surfaced internal emails and a tape-recorded employee call — one UHC nurse said on the call "we're still gonna say no" despite the treating physician's instructions. UnitedHealthcare settled within weeks of ProPublica publishing the story.
Eric Tennant, West Virginia dad — approval came after he was too sick to receive it
KFF Health News + West Virginia Watch, 2024–2025
Tennant, 58, a coal-mining safety instructor from Bridgeport, West Virginia, was diagnosed in early 2025 with a rare bile-duct cancer. His doctors recommended histotripsy — a $50,000 non-invasive ultrasound tumor ablation. His insurer, the state Public Employees Insurance Agency (administered by UnitedHealthcare), repeatedly denied coverage as "not medically necessary." The carrier reversed course in May 2025 only after KFF Health News and NBC News submitted questions, but by then Tennant had deteriorated past the point of being a candidate. He died on September 17, 2025. In 2026 West Virginia's governor signed a prior-authorization reform law citing his case.
The insurer controlled the record of what happened. The patient did not.
Every case above turned on what the portal, the denial letter, the chart, or the phone call said at the time — and on whether the patient or their estate could prove it later. In each one, the insurer was the sole custodian of that record. Discovery, depositions, ProPublica investigations and class-action subpoenas eventually surfaced the truth — but only for the rare patient with attorneys willing to fight for years.
A $4.99 SnapPack at the moment of the original portal interaction — the prior-auth approval, the EOB, the chat transcript, the visit summary — gives you a copy the insurer cannot edit, archive, or "forget." Bitcoin-blockchain-timestamped. SHA-256 hashed. Independently verifiable. Self-authenticating under FRE 902(13)/(14).
Don't miss the deadline — it forecloses the appeal
Health insurance appeal deadlines by insurer (US 2026)
Missing the internal-appeal deadline waives your right to escalate. Deadlines vary sharply by carrier and plan type — check the denial letter for the exact date and confirm in your member handbook.
Insurer / Plan
Internal appeal deadline
External review (IRO) deadline
Notes
ACA Marketplace (HealthCare.gov)
180 days from denial
4 months after internal denial
Federal floor; some plans grant more time
Aetna (commercial)
180 days
4 months
Urgent care: 72-hour expedited
Anthem / Blue Cross Blue Shield
180 days
4 months
Plan-specific variations by state
Cigna (commercial)
180 days
4 months
EviCore prior-auth screening — capture early
UnitedHealthcare
65 days (much shorter)
4 months
All plan types; nH Predict / NaviHealth screening
Humana (commercial & MA)
60 days
4 months
Tighter than ACA floor
Molina Healthcare
60–180 days (plan/state-dependent)
State fair-hearing process
~24% denial rate, highest among major plans
Medicare Advantage (all insurers)
60 days for reconsideration
Five-level CMS process
~80% of appeals overturned (HHS OIG)
Medicaid
60–90 days (varies by state)
State fair-hearing
Check state-specific managed-care rules
ERISA (employer-sponsored)
180 days
Federal court after admin appeal
29 CFR 2560.503-1; LTD plans on similar timeline
No Surprises Act (surprise bill)
120 days for IDR dispute
Independent Dispute Resolution
$400+ over Good Faith Estimate triggers
Sources: ACA Section 2719 · 29 CFR 2560.503-1 (ERISA) · CMS Medicare Advantage appeal rules · Muni Health 2026 deadline summary · KFF 2024 analysis. Confirm your denial letter and plan documents for the exact deadline applicable to your case.
Decode your denial letter
Common US health insurance denial reason codes — meaning, appeal odds, and evidence checklist
Every denial letter cites a Claim Adjustment Reason Code (CARC) such as CO-50 or CO-197. The code dictates how appealable the denial is and which evidence will overturn it. Find your code below.
Code
Meaning
Appeal odds
Evidence that wins
CO-50
"Not medically necessary" — most common appealable denial. Insurer disputes clinical justification.
Sources: X12 / WPC Edit Master CARC & RARC code list · CMS Medicare Claims Processing Manual · X12.org reason codes. Your denial letter typically includes both a CARC (CO/PR) and a RARC (N/M) code — cite both verbatim in your appeal letter.
Got denied today?
Your next 30 minutes — from denial letter to appeal filed
A weekend-doable plan combining ProofSnap (evidence) with a free AI appeal tool (Counterforce Health). Total cost: $4.99. Total time: ~30 minutes once you have your denial letter.
1
Install ProofSnap & buy SnapPack
~3 min · $4.99
Chrome Web Store → Add to Chrome → pay inside the extension. Card required at checkout (standard Stripe).
2
Capture 4 pages in your insurer portal
~7 min · 4 captures
(a) Denial letter with full reason codes · (b) Original prior-auth approval (if any) · (c) EOB / claim detail page · (d) MyChart visit summary linked to the denied service. Each capture = one forensic ZIP.
Upload your denial letter PDF + your insurance policy document. The AI analyzes both and drafts a customized appeal letter citing the specific clinical criteria. Mayo Clinic experts published this workflow; Counterforce reports ~70% overturn rate.
4
Review & customize the AI-drafted appeal
~8 min
AI can hallucinate medical details — double-check every clinical claim against your actual records. Add a paragraph in your own voice describing daily impact.
5
Send the appeal — with your ProofSnap ZIPs attached
~2 min
Email or upload to your insurer's appeal address (listed on the denial letter). Reference the ZIP filenames in your letter: "Exhibit A — prior-authorization approval, captured [date] with cryptographic timestamp verifiable at opentimestamps.org." The insurer cannot disclaim what your blockchain timestamp proves was on their portal.
After you file: federal ACA rules require the insurer to decide within 30 days (pre-service) or 60 days (post-service). Urgent care: 72 hours. If denied again, you have 4 months to request an external IRO review — reuse the same captures. If you have an active treatment that cannot wait: file the urgent appeal AND start the IRO request in parallel — federal rules allow it.
Fighting an ongoing multi-month case (multiple appeals, IRO, bad-faith)? See which plan.
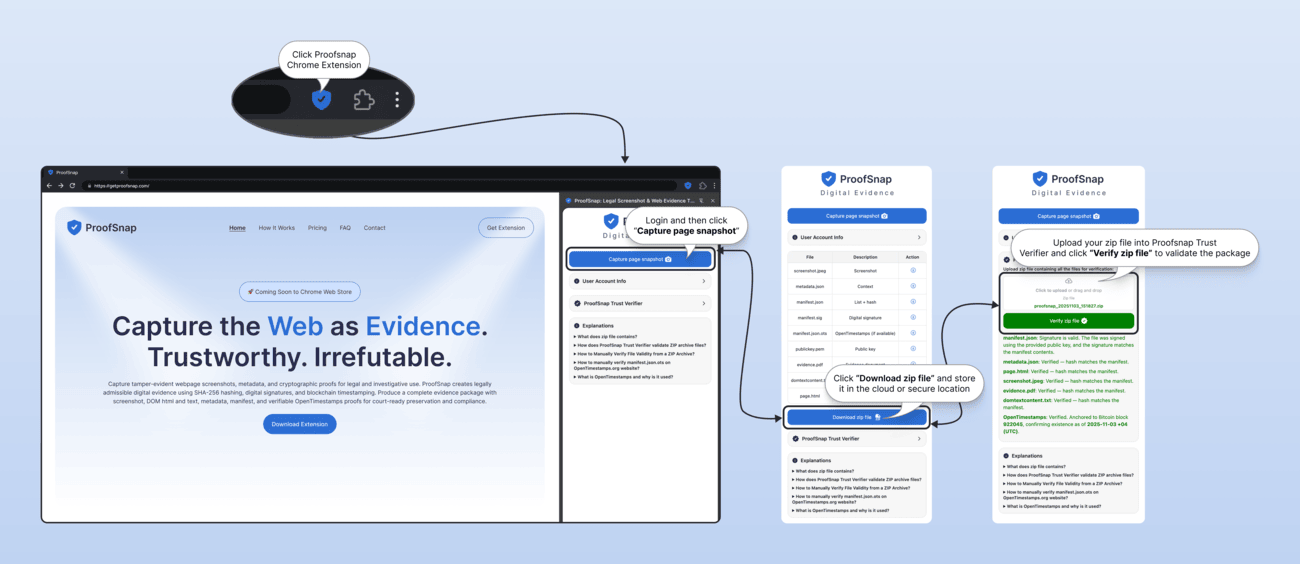
From zero to first portal capture — under 2 minutes
No technical skills required. No advocate fees. Just 3 clicks.
What happens after you click
From click to your first portal capture: under 2 minutes
1Chrome Web Store opens · click "Add to Chrome"
2Pay $4.99 inside the extension
3Open MyChart, your EOB page, or insurer portal and click the icon
4Download your forensic ZIP · attach to your appeal letter or send to your advocate
Capture this evidence today. The portal can change tomorrow.
Insurance portals are dynamic. Approval statuses change. EOBs get updated. Prior-auth letters get archived. What the portal said in March may not be what it says in June. Capture first. Decide later whether you'll need it.
Your US patient evidence checklist:
Urgent care? Pre-service and concurrent-care appeals must be decided within 72 hours under federal rules. Capture the denial letter and your provider's medical-necessity statement before filing — the appeal clock does not stop while you gather evidence. Authenticated captures attached to your appeal letter close the loop in one shot.
Do the math:
$0
Recovered without an appeal
$4.99
SnapPack (10 captures)
$1K–$50K+
A single denied GLP-1, IVF cycle, or out-of-network bill
A patient advocate charges $75–$200/hour. A bad-faith attorney charges $300+/hour. ProofSnap: $4.99 one-time.
Install takes 30 seconds. First capture in under 2 minutes.
The 2026 healthcare reality
Insurance AI denies you. Patient AI appeals for you. Both need the same thing: authenticated source documents.
2024–2026 saw an explosion of AI tools on both sides — nH Predict, EviCore, Optum on the insurer side; Counterforce Health, Claimable, and ChatGPT workflows on the patient side. The bottleneck is no longer drafting appeal letters. It is feeding those tools authenticated, timestamped evidence the insurer cannot disclaim.
The insurer side
Algorithmic prior-auth denials within seconds — nH Predict (UnitedHealth), EviCore, Optum. Class actions allege denials without human review.
Portal status changes from "Approved" to "Pending" without notification
All three need the same thing: the original denial letter, prior-auth approval, EOB and portal correspondence — authenticated so they cannot be disputed
Where ProofSnap fits
The evidence layer your AI appeal tool is missing
1
Capture with ProofSnap
SnapPack each portal page, denial letter, EOB, prior-auth approval. Each ZIP is sealed with SHA-256 + Bitcoin blockchain timestamp.
2
Feed text to your AI tool
Paste the evidence.pdf and EOB content into Counterforce, Claimable, or ChatGPT. AI generates the appeal letter in under a minute.
3
Attach the ZIPs to the appeal
The AI-written letter cites authenticated exhibits. The IRO reviewer sees timestamped evidence that the insurer cannot claim "was edited" or "never said that."
Important caveat for AI tools: ChatGPT and most general-purpose AIs are not HIPAA-compliant. Strip identifiers before pasting, or use a purpose-built privacy-oriented tool like Counterforce Health. ProofSnap captures stay on your device — no PHI ever leaves your browser regardless of which AI tool you pair with.
The single most common red flag in patient-side malpractice cases. EHR audit trails (Epic, Cerner, MEDITECH, athenahealth) record who-changed-what-when — but your independent capture is what proves the original content the chart said before the amendment.
The risk
Providers can "supplement" charts via HIPAA-compliant amendment process — properly dated, it is legal.
Undated, post-incident changes — the kind that hide an error — are spoliation, with severe sanctions.
Once juries see a chart alteration, credibility collapses — verdicts up to $20M have followed.
But proving alteration requires comparing the current chart to what the chart said earlier — that is your job.
The defense
Capture MyChart the day of every visit — visit summary, plan of care, medications, vital signs, lab orders.
Your ProofSnap timestamp is independently verifiable on the Bitcoin blockchain — the provider cannot dispute when you captured.
If the chart later differs from your capture, your attorney can demand the EHR audit trail and prove spoliation.
Spoliation triggers adverse-inference jury instructions — the jury is told to assume the alteration was unfavorable to the defense.
Practical rule: if you experienced anything that could become a complaint — a missed diagnosis, an adverse drug reaction, a procedure complication, an unexplained handover — SnapPack your MyChart visit summary the same day. You do not have to decide whether to act. You just have to preserve the option. Once the chart is amended, recovery of the original content requires litigation discovery and an expensive expert witness.
Which denial or dispute are you fighting?
Nine high-cost patient scenarios where authenticated capture is the difference
Each row maps a common dispute type to the specific portal pages, letters, and visit recordings that win appeals, IRO reviews, and bad-faith cases.
GLP-1 / Obesity meds
Zepbound, Wegovy, Mounjaro, Ozempic denials
60–80% of appealed GLP-1 denials are overturned (rising to ~85% with strong medical documentation). The bottleneck is documented weight history and lifestyle-intervention evidence.
What to capture:
MyChart weight history (6–12 months minimum)
Nutritionist visit notes, gym membership records, documented diet program logs
Prior-auth request submitted by your prescriber + the denial reason codes
Peer-to-peer review call (Video SnapPack) — your prescriber's voice arguing medical necessity is powerful at IRO level
IVF / Fertility
IVF cycle, egg freezing, and fertility-preservation denials
A single denied IVF cycle is $15K–$30K out of pocket. Coverage rules differ wildly by state mandate and employer plan.
What to capture:
Summary of Benefits and Coverage (SBC) section on fertility
Pre-treatment quote vs. final EOB — gaps prove bait-and-switch
State-mandate citations (IL, MA, NY, NJ, RI and others) attached to your appeal
Member-services chat transcripts (each reference number captured with timestamp)
Gender-affirming care
Hormone therapy, surgery, and mental-health letter denials
Coverage continues to shift state-by-state. WPATH-aligned medical-necessity documentation routinely wins appeals when properly authenticated.
What to capture:
Mental-health provider letters of medical necessity
Plan documents and SBC sections that explicitly cover or exclude the procedure
Discriminatory denial reason codes (cited verbatim in your appeal)
State insurance commissioner / OCR complaint references
~65–70% of telemedicine malpractice cases involve misdiagnosis. Most telehealth platforms purge chat logs and recordings within days.
What to capture (Video SnapPack):
The visit itself: video, audio, chat (legality depends on your state — see consent map below)
Post-visit summary in MyChart and the provider's clinical note (often inconsistent with what was said)
Prescription / refill history and any refused referral records
Discharge / aftercare instructions presented at the end of the visit
Disability / LTD
Long COVID, ME/CFS, fibromyalgia, chronic pain LTD denials
LTD carriers (Unum, Hartford, MetLife) routinely deny subjective-symptom claims for "lack of objective evidence." ERISA appeals run on 180-day clocks — documentation density wins.
What to capture:
MyChart daily symptom logs and patient-reported outcomes (PROMIS scores)
Specialist evaluations: infectious disease, pulmonology, cardiology, neuropsychology — both clinical notes and portal messages
CPET / two-day cardiopulmonary exercise test results (objective evidence of post-exertional malaise)
LTD insurer portal communications — every "request for additional information" timestamped
ER misdiagnosis
Wrong diagnosis, premature discharge, missed stroke / sepsis / MI
Pre-formatted ED discharge templates routinely print the wrong diagnosis. ~40% of patients misunderstand discharge instructions — and the printed paper is the document the hospital points to.
What to capture (same day — before any amendment):
The ED physician's note — especially the differential diagnosis section
If you returned within 72 hours with a worse condition: the second visit's record proves the missed diagnosis
Mental health & Workers' comp
Therapy records disputes, workplace-injury denials
State workers' comp portals (CA EAMS, NY eClaims, VA WebFile, federal SEAPortal) and behavioral-health platforms (TheraNest, SimplePractice, BetterHelp) follow the same purge pattern as health portals.
What 2026 US health-insurance appeal data actually shows
The framework rewards appealing. The failure mode is having no preserved record of what the insurer said.
80%
Medicare Advantage appeal overturn rate — CMS / HHS-OIG data shows roughly 80% of appealed prior-authorization denials are partially or fully overturned. The denial rate has been rising but appeal overturn rates remain high — meaning the majority of initial denials are wrong on the merits.
Source: HHS Office of Inspector General OEI-09-19-00350.
44%
ACA internal appeal success rate — KFF analysis of 2023 ACA marketplace data shows fewer than 1% of denied claims were appealed; of those that were, 44% of internal appeals overturned the denial. The system rewards persistence backed by evidence.
Source: KFF, "Claims Denials and Appeals in ACA Marketplace Plans in 2024."
82%
Of prior-authorization denials overturned 2019–2023 — nearly 82% of prior-authorization denials in this window were partially or fully overturned upon appeal. The bottleneck is patients not having authenticated evidence of the original approval or the denial reason codes.
Of US medical bills contain errors — industry studies from Medical Billing Advocates of America and patient-advocate organizations estimate 49–80% of medical bills contain at least one error, with up to 8 in 10 hospital bills affected. Itemized statements captured with timestamps are the foundation of every dispute.
Source: Medical Billing Advocates of America; Patient Advocate Foundation.
Why your iPhone screenshot is not enough for an IRO or bad-faith case
Independent Review Organizations, ERISA appeal panels, state insurance commissioners, and bad-faith litigators look for the same authentication that federal courts require under FRE 901(a). A bare PNG file does not pass the test.
Your phone screenshot
No independent timestamp — EXIF can be edited
Fabricated in 30 seconds with Inspect Element
No URL verification, no HTML source
No chain of custody documentation
Insurer can claim the page "never said that"
May require expert witness ($5K–$15K) to authenticate
ProofSnap evidence package
OpenTimestamps blockchain anchor (Bitcoin)
SHA-256 hash — any tampering detected instantly
Full metadata: URL, IP, headers, TLS certificate, cookies
Forensic log + chain of custody documentation
Up to 15 forensic files per capture (plan-dependent)
Meets FRE 901(b)(9) process authentication
Self-authenticating under FRE 902(13) + 902(14)
Legal basis: FRE 901(a) authentication · FRE 901(b)(9) process authentication · FRE 902(13) certified records of an electronic process · FRE 902(14) certified digital data · 45 CFR 164.524 HIPAA right of access
The HIPAA question every patient asks
"Am I allowed to do this?"
Short answer: yes. HIPAA regulates providers, plans, and clearinghouses — not patients capturing their own records for their own use.
You are the data subject
HIPAA's privacy and security rules apply to "covered entities" (hospitals, doctors, insurers, clearinghouses) and their "business associates." When you log into MyChart as the account holder, you are capturing your own information for your own use. HIPAA does not regulate that.
Under 45 CFR 164.524, you have an explicit federal right to access your own records.
Your data stays on your device
ProofSnap captures everything client-side in your Chrome browser. The screenshot, HTML, metadata, and forensic ZIP never leave your computer.
The only data sent to a ProofSnap server is the SHA-256 hash of your evidence file — a non-reversible cryptographic fingerprint forwarded to OpenTimestamps for blockchain anchoring. The hash is not PHI; it cannot be reversed to recover the original content.
Patient advocates & attorneys
With your written HIPAA authorization — or as your designated "personal representative" under HHS guidance — a patient advocate, claims advocate, healthcare power-of-attorney holder, or plaintiff-side attorney has the same access rights as you.
They do not become a HIPAA "business associate" simply by helping you. BA status applies to vendors of covered entities, not patient-side representatives.
FRE 901 & 902 self-authentication
FRE 901(b)(9) allows authentication through "evidence describing a process or system and showing that it produces an accurate result." SHA-256 + OpenTimestamps + chain of custody is exactly that.
FRE 902(13) certifies records of an electronic process. FRE 902(14) certifies data taken from an electronic system. ProofSnap's package was designed against these standards.
Bottom line: capturing your own portal pages, EOBs, and visit summaries is something every patient is legally entitled to do. Doing it with cryptographic timestamps is what turns "I remember it said approved" into evidence that wins an appeal. This page is general information, not legal advice — consult a licensed attorney in your state for your specific case.
Can I record my telehealth visit or peer-to-peer review?
US recording-consent map — one-party vs. all-party states
Recording a phone or video conversation is governed by state wiretap statutes. 38 states + DC let you record with only your own consent. Approximately 11–13 states require all parties to consent (the list varies by interpretation of mixed-rule states).
One-party-consent (38 states + DC)
You can legally record your own telehealth visit or peer-to-peer call without notifying the provider or insurer. Best practice: still ask first — but legally you are covered.
Both parties must consent. Ask the provider before clicking record, and capture their verbal consent on the recording itself. Most platforms (Zoom for Healthcare, Doxy.me) display an in-app consent banner that satisfies the rule.
States: California, Delaware (mixed), Florida, Illinois, Maryland, Massachusetts, Michigan, Montana, New Hampshire, Oregon, Pennsylvania, Washington. Connecticut and Nevada have mixed/conditional rules depending on context.
Even in all-party states, the screen content itself — chat messages, displayed clinical notes, slide decks during peer-to-peer review — can typically be captured without recording consent because it is information shown to you, not a conversation. Video SnapPack handles both modes (with or without audio). Always confirm specifics with a licensed attorney in your state.
For your patient advocate or attorney
What your advocate sees when you hand them the ZIP
You do not have to explain blockchain timestamps or SHA-256 hashing. The evidence package speaks for itself in the language your advocate or attorney already uses every day.
Plain-English summary your advocate will recognize immediately:
✓
Forensic evidence package per capture
Up to 15 files: screenshot, full HTML, DOM snapshot, PDF report, metadata JSON, forensic log, chain of custody, signed manifest, capture video (Enterprise).
✓
Meets FRE 901(b)(9) process authentication
"Evidence describing a process or system and showing that it produces an accurate result." Citable in an appeal letter, IRO submission, or bad-faith complaint.
✓
Self-authenticating under FRE 902(13) + 902(14)
Certified records of an electronic process and certified digital data can be admitted without a live forensic expert — saving $5K–$15K in expert-witness fees.
✓
Independently verifiable blockchain timestamp
OpenTimestamps anchors the SHA-256 hash to Bitcoin. Anyone can verify the timestamp at opentimestamps.org — no ProofSnap involvement needed.
Hand your advocate this exact sentence:
"This is a forensic capture package with SHA-256 hashing, OpenTimestamps blockchain anchoring, and a chain of custody document. It is designed to meet FRE 901(b)(9) process authentication and self-authenticate under FRE 902(13) and 902(14). The evidence.pdf and manifest.json contain everything you need for the internal appeal, IRO submission, or bad-faith complaint."
Start capturing your evidence today
One-time $4.99. No subscription. Use tonight.
Built for patients in the middle of a denial, not a compliance department. Buy once, capture 10 portal pages, attach the ZIP to your appeal letter.
Recommended for one denial
$4.99one-time
SnapPack — 10 forensic captures
No subscription. Pay once, done.
Credits never expire. Use them tonight or next month.
Forensic ZIP per capture — screenshot, HTML, metadata, SHA-256 hash, blockchain timestamp
FRE 901(b)(9) admissible — all 50 states, IROs, ERISA panels
Card required at checkout — standard Stripe payment
For telehealth visits, peer-to-peer reviews, MyChart walkthroughs
Record the entire browser window with audio — Zoom for Healthcare, Doxy.me, Teladoc, Amwell, Cigna / UnitedHealthcare / Aetna member portal calls — sealed with cryptographic timestamps.
Up to 30 minutes per video (Enterprise)
Audio + screen + chat in one .webm container
Each video sealed with SHA-256 hash + blockchain timestamp
Bundled eIDAS qualified credits for extra-strong stamping
Recording is governed by state wiretap statutes — see the one-party / all-party map above before pressing record.
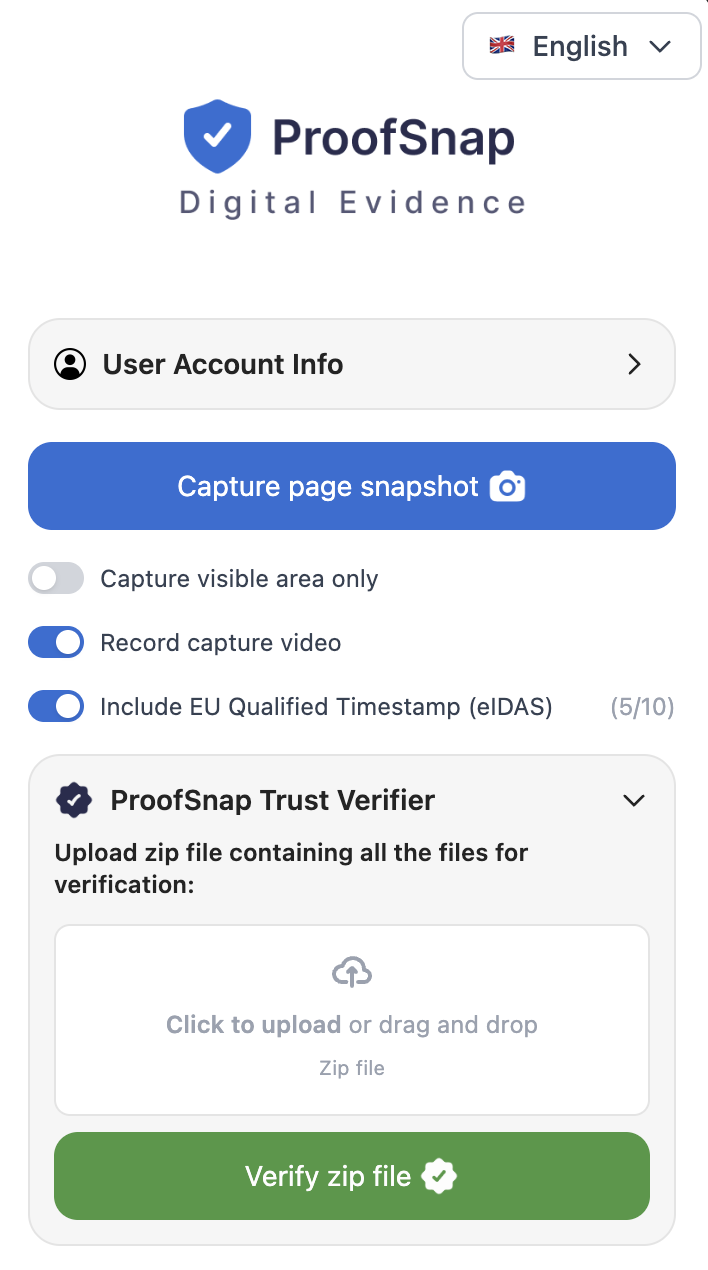
Want to verify a captured ZIP? Open the Trust Verifier — drag a full ZIP and check hash, signature, blockchain timestamp.
Patient evidence FAQ — United States
Yes. HIPAA regulates "covered entities" — hospitals, doctors, insurers, clearinghouses — and their "business associates." It does not regulate patients capturing their own medical or insurance information for personal use. Under HIPAA's individual right of access (45 CFR 164.524), you are entitled to your own records. When you log into MyChart, FollowMyHealth, or your insurer portal as the account holder, you are the data subject. ProofSnap captures stay on your device; only a non-reversible SHA-256 hash is sent to OpenTimestamps for blockchain anchoring — no PHI ever leaves your browser.
Very high — but almost no one tries. KFF analysis of 2023 ACA marketplace data shows fewer than 1% of denied claims were appealed, yet of those that were, 44% of internal appeals overturned the denial. For Medicare Advantage prior-authorization denials, CMS data shows approximately 80% of appealed denials are partially or fully overturned. For GLP-1 medications such as Wegovy and Zepbound, 60–80% of appealed denials are overturned (rising to ~85% with strong medical documentation). The bottleneck is not whether appeals win — it is whether patients have authenticated evidence of what the insurer originally said.
Yes. The federal No Surprises Act (effective January 2022) protects you from surprise bills for emergency care and certain non-emergency out-of-network services at in-network facilities. If your final bill is more than $400 above a Good Faith Estimate you received, you have 120 days to file an Independent Dispute Resolution (IDR) request through the patient-provider dispute resolution process. You will need to submit the Good Faith Estimate, EOB, itemized statement, and supporting communication — all timestamped. ProofSnap captures each piece with cryptographic proof of when you received it.
Under federal ACA rules, you have 180 days from the date of the denial letter to file an internal appeal with your insurer. Some plans grant shorter windows for urgent care or pre-service appeals (as fast as 72 hours). After the internal appeal, you have 4 months to request an external review by an Independent Review Organization (IRO). ERISA plans (most employer-sponsored coverage) have similar but technically distinct timelines under 29 CFR 2560.503-1. Capture everything immediately — portals routinely change content, and recovering "what the page said in February" is much harder than capturing it today.
It depends on your state. 38 US states plus DC follow the "one-party consent" rule — only one party to the conversation must consent. In those states, you can legally record your own telehealth visit without notifying the provider (though most ethics guidance recommends asking). Approximately 11–13 states are "all-party consent" (the list varies by interpretation of mixed-rule states): commonly classified all-party states include California, Florida, Illinois, Maryland, Massachusetts, Michigan, Montana, New Hampshire, Oregon, Pennsylvania, and Washington; Connecticut, Delaware, and Nevada have mixed or conditional rules. In all-party states, both you and the provider must consent. Recordings made legally in your jurisdiction are generally admissible in court. ProofSnap's Video SnapPack captures the entire browser window with cryptographic timestamps and chain of custody. Confirm your state's rule before recording.
An iPhone or Android screenshot is a single image file with no independent timestamp, no URL verification, no HTML source, and no chain of custody. The insurer's attorney can argue it was edited, fabricated, or pulled from a different page. Under FRE 901(a), you must authenticate that the screenshot is what you claim. ProofSnap creates a forensic ZIP package (up to 15 files depending on plan) with SHA-256 hash, OpenTimestamps blockchain timestamp anchored to Bitcoin, full page HTML, metadata, signed manifest, and chain of custody — meeting FRE 901(b)(9) process authentication and self-authenticating under FRE 902(13) and 902(14).
This is exactly why authenticated capture matters. Insurer portals are dynamic web pages — content can be edited, statuses can change from "Approved" to "Pending" without notification, and prior approval letters can be archived or removed. Once captured with ProofSnap, the page is fixed in time. The Bitcoin blockchain timestamp is independently verifiable — anyone (your insurer, your attorney, an arbitrator, an IRO reviewer) can confirm at opentimestamps.org that the SHA-256 hash existed at the block height stamped. The insurer cannot retroactively claim the page never said what it said.
Yes. GLP-1 denials are one of the highest-volume appeal categories in 2026 — roughly 62% of GLP-1 requests were denied in 2024. Published 2025–2026 data shows 60–80% of appealed GLP-1 denials are overturned, with success rates approaching 85% when supported by strong medical documentation. Key evidence: your weight history in MyChart (6–12 months documented), records of lifestyle interventions (nutritionist visits, gym membership, diet program logs), the prior-authorization request submitted by your prescriber, the denial letter with specific reason codes, and any portal correspondence with the plan. Capture each portal page with ProofSnap so timestamps are independent — powerful evidence if a peer-to-peer review or external IRO appeal becomes necessary.
Yes. With your written HIPAA authorization (or as your designated "personal representative" under HHS guidance), a patient advocate, claims advocate, healthcare power-of-attorney holder, or plaintiff-side attorney has the same record-access rights as you. They do not become a HIPAA "business associate" simply by helping you — that designation applies to vendors of covered entities, not patient-side representatives. Advocates can capture portal pages, EOBs, and correspondence with the same forensic rigor. Many use a Professional or Enterprise plan to cover multiple clients per month.
Yes. Federal Rules of Evidence 901(b)(9) explicitly allows authentication through "evidence describing a process or system and showing that it produces an accurate result." SHA-256 hashing plus OpenTimestamps blockchain anchoring plus chain of custody documentation is exactly that. FRE 902(13) allows certified records of an electronic process to self-authenticate without a live witness. FRE 902(14) allows certified copies of data taken from an electronic device or system to self-authenticate. ProofSnap's evidence package was designed against these standards. State courts that mirror the federal rules (most do) accept the same framework. Discuss with your bad-faith or ERISA attorney.
The framework is similar but the timelines and forms differ. Medicare Advantage organization determinations can be appealed in five levels: reconsideration by the plan, IRE (Independent Review Entity) reconsideration, OMHA Administrative Law Judge hearing, Medicare Appeals Council review, and federal district court. CMS data shows roughly 80% of appealed prior-authorization denials are overturned. Medicaid appeals go through state fair-hearing processes — timelines vary by state but generally 60–90 days to request. Authenticated portal captures, EOBs, and correspondence are admissible at every level. The federal Office of Medicare Hearings and Appeals routinely accepts electronically authenticated exhibits.
No — for internal appeals and IRO requests you do not need a lawyer. The federal ACA framework is designed for patients to self-appeal. Free resources include the State Health Insurance Assistance Program (SHIP), the Patient Advocate Foundation, and Dollar For. However, appeals filed with advocate help succeed roughly 80% of the time, compared with just 11% for patients who appeal entirely on their own (Patient Advocate Foundation). Authenticated evidence is the single biggest factor your advocate or attorney needs — and the single biggest reason DIY appeals fail.
Yes. Open the Trust Verifier in any browser, drag your full evidence ZIP onto the drop zone, and the verifier independently checks the SHA-256 hash, the signed manifest, the OpenTimestamps blockchain proof, and the chain of custody — no ProofSnap account or login required. The verifier accepts the entire ZIP package, not individual files. Anyone with the ZIP (your advocate, attorney, IRO reviewer, insurer) can run the same verification.
Yes — they pair extremely well. Counterforce Health (free, ~70% reported overturn rate, University of Pennsylvania + NIH funded), Claimable (~$40 per appeal), and ChatGPT / Gemini with Mayo Clinic-published prompts all generate appeal letters in under a minute. None of them solve the evidence problem — they need authenticated source documents to cite. ProofSnap provides exactly that. Workflow: SnapPack each portal page and denial letter, paste the text into your AI tool, attach the timestamped ZIPs to the appeal letter the AI generates. HIPAA caveat: ChatGPT is not HIPAA-compliant. Strip identifiers before pasting, or use Counterforce Health (purpose-built and privacy-oriented).
Providers are allowed to supplement charts — if they clearly date the entry to reflect it was added after-the-fact, it is legal under HIPAA. Undated, post-incident alterations to hide an error are spoliation, with severe sanctions. Modern EHRs (Epic, Cerner, MEDITECH, athenahealth) maintain automatic audit trails recording every access and edit. In a malpractice case, your attorney can subpoena the audit trail and ask the court for an adverse-inference instruction — the jury is told to assume the alteration was unfavorable to the defendant. One key piece of evidence is missing from the audit trail though: the exact pre-amendment text. That is where your ProofSnap capture (taken the day of the visit, blockchain-timestamped) becomes the spoliation case's foundation. Verdicts up to $20M have followed proven chart alterations.
Long-Term Disability carriers (Unum, Hartford, MetLife, Cigna LINA, Prudential) routinely deny Long COVID, ME/CFS, fibromyalgia, and chronic-pain claims for "lack of objective evidence of functional impairment." Federal appellate courts have repeatedly affirmed such denials — including a March 2026 Second Circuit decision and a Sixth Circuit ruling upholding Unum's denial of a nurse's Long COVID claim. Winning the appeal requires documentation density: contemporaneous MyChart symptom logs, PROMIS scores, specialist evaluations from infectious disease / pulmonology / cardiology / neuropsychology, and ideally a two-day CPET (cardiopulmonary exercise test) showing post-exertional malaise. Under ERISA you typically have 180 days from the denial letter to file the administrative appeal — missing it forecloses the lawsuit. Capture every portal page, every "request for additional information," and every IME letter with ProofSnap so the timeline is unimpeachable.
Wrong-diagnosis discharges from busy EDs are a documented pattern — pre-formatted disease-specific discharge templates make a single click of the wrong diagnosis create a paper trail that contradicts what the physician actually evaluated. Cases of patients sent home with one-sided facial droop and motor weakness (a classic stroke) misdiagnosed as a neurogenic disorder have been litigated for millions. Step one: SnapPack the MyChart ED visit summary today — printed diagnosis, instructions, prescriptions, ordered/reviewed labs, the ED physician's note (especially the differential-diagnosis section), and triage vitals. If you returned to an ED within 72 hours with a worse condition, capture that second record too. Step two: consult a medical-malpractice attorney — statutes of limitations for misdiagnosis cases run as short as 1–2 years depending on state.
Yes. State workers' comp systems run on online portals — California EAMS, New York eClaims, Virginia WebFile, federal SEAPortal — that behave identically to health-insurance portals: status changes silently, communications are archived, and "we never received that document" is a common defense. Substantial evidence in a workers' comp claim includes medical records, lab tests, expert opinions, witness testimony, photographs of the accident scene, dated HR communications, employer accident-report forms, and IME (Independent Medical Examination) request letters. Dated screenshots and timestamped contemporaneous notes are central — especially when HR or the insurer gave you verbal information that turns out to differ from the written record. ProofSnap captures each portal page or HR communication with a blockchain timestamp that an administrative law judge can verify independently.
Algorithmic / AI-assisted prior-authorization denials are a major 2024–2026 litigation front. UnitedHealth's nH Predict tool, EviCore, and Optum have all been named in class actions alleging Medicare Advantage denials issued without meaningful human review — some in seconds. State insurance departments and CMS are tightening rules requiring "case-by-case clinical determination by a qualified physician." When you receive a near-instant denial, capture the timestamp visible in the portal — the gap between submission and denial is precisely the evidence regulators and class-action attorneys need. Capture the denial letter text, the reason codes, and any "peer reviewed by" signature. Save the portal status-change timeline. These captures are admissible in both the internal appeal and, if it gets there, the lawsuit.
Insurance "bad faith" is a tort claim available in most states (plus statutory unfair-claims-practices laws like California Unfair Insurance Practices Act, Texas Insurance Code Ch. 541, Florida Stat. 624.155). To win you must show (1) benefits due under the policy were withheld and (2) the reason for withholding was unreasonable. The evidence that wins: a documented timeline of insurer conduct — every "we will get back to you," every reference number, every status change, every denial inconsistent with prior approvals. Most patients lose bad-faith cases because they cannot reconstruct the timeline. ProofSnap captures freeze each interaction with the blockchain timestamp, building a contemporaneous record that becomes powerful evidence of unreasonable delay, misrepresentation, or denial without basis.
A winning appeal letter has six elements: (1) your full name, plan ID, claim number, and date of denial; (2) the specific clinical service, procedure, or medication denied; (3) the exact denial reason and reason code copied verbatim from the denial letter; (4) a point-by-point rebuttal of each cited reason — with medical-necessity citations, treating-physician statements, and clinical guidelines (e.g., AGA, ASCO, ACS, FDA labeling); (5) the relief requested (overturn the denial and authorize service); (6) attached evidence — prior-authorization approval, medical records, lab results, physician letters, and authenticated portal captures. In 2026, free AI tools draft this in under a minute: Counterforce Health (free, ~70% overturn rate, University of Pennsylvania + NIH funded), Claimable (~$40 per appeal), and ChatGPT or Gemini with Mayo-Clinic-published prompts. ProofSnap provides the authenticated source documents your AI tool needs to cite.
Deadlines vary significantly by carrier. ACA marketplace, Aetna, Anthem/BCBS, Cigna, Premera, and ERISA employer plans give you 180 days from the denial letter to file an internal appeal. UnitedHealthcare is shorter at 65 days for all plan types. Humana gives 60 days. Medicare Advantage allows 60 days for reconsideration regardless of insurer (CMS rule). Medicaid varies state-by-state, typically 60–90 days. Urgent-care or pre-service appeals may grant only 72 hours expedited review. After the internal appeal, you have 4 months to request an external review by an Independent Review Organization. The No Surprises Act gives you 120 days for Independent Dispute Resolution on surprise bills $400+ over a Good Faith Estimate. Confirm in your denial letter — missing the deadline forecloses your right to appeal. See the full deadlines table for all carriers.
Prior authorization (PA, also called pre-authorization or precertification) is an approval an insurer requires before it will cover certain medications, procedures, or services. Your prescriber submits a PA request with clinical justification, and the insurer responds approve, deny, or request additional information. PA is the highest-volume denial category in 2026 — over 80% of appealed PA denials are overturned per CMS and AMA data, yet fewer than 1% of patients ever appeal. Common targets: GLP-1 medications (Zepbound, Wegovy, Ozempic, Mounjaro), biologics, oncology drugs, advanced imaging (MRI, PET), IVF, gender-affirming care, transplant evaluation, mental-health intensive outpatient programs. Insurers are increasingly using algorithmic screening (UnitedHealth's nH Predict, EviCore, Optum) — class-action litigation alleges denials issued without meaningful human review. Capture the PA approval letter when issued and screenshot the portal status — insurers routinely "forget" the approval at claim-payment time.
The process is similar across major US insurers but the deadlines and submission addresses differ. For UnitedHealthcare you have 65 days (much shorter than other carriers) — submit via the member portal, fax, or certified mail with claim number, denial letter, and supporting documentation. Aetna, Cigna, and Anthem/BCBS all give 180 days for commercial plans. Each insurer publishes its appeal address and forms in the denial letter and member handbook. Critical: capture screenshots of the member portal showing the denial timeline, any "approved then reversed" status, and member-services chat transcripts before the carrier archives them (typically within weeks). Use Counterforce Health to draft the letter, attach the ProofSnap-authenticated portal evidence, and submit by certified mail with return receipt. If the internal appeal is denied, escalate to your state insurance department external review (IRO) within 4 months — 38–53% of external reviews overturn the denial.
No subscription · HIPAA-clear · Admissible in all 50 states under FRE 901
About this guide
Authorship, methodology, and editorial review
Author & Editor
Radim Motycka
Founder and Lead Engineer, ProofSnap. Blockchain engineer with 10+ years in cryptographic protocol design. Integrated eIDAS qualified timestamps (Disig a.s., EU Regulation 910/2014) and OpenTimestamps Bitcoin anchoring into ProofSnap's evidence pipeline.
Every statistic cites the originating institution and year
Case studies link to named court dockets and primary investigative reporting
Updated as deadlines, statutes, and litigation evolve (monthly review)
Important disclaimer
Not medical or legal advice
This guide is editorial content for informational purposes only. It is not medical advice, legal advice, or a substitute for consultation with a licensed physician, attorney, or licensed patient advocate in your state.
Individual results depend on jurisdiction, plan terms, treating physician documentation, and procedural compliance. The author is not a licensed physician, attorney, or insurance broker. For a denial appeal or coverage dispute affecting your health, consult a licensed professional. For urgent care needs, call your provider or 911.
Editorial timeline: First published May 17, 2026 · Last reviewed and updated May 18, 2026 · Next scheduled review: monthly. Spotted an error or outdated statistic? Email support@getproofsnap.com.
Affiliations & conflicts of interest: ProofSnap sells the forensic-evidence Chrome extension recommended in this guide. We do not receive referral fees from Counterforce Health, Claimable, patient-advocate organizations, or any insurer. All third-party tool mentions are based on publicly verifiable performance data.